For yours truly, only adjustability will do.
James Davies had seen enough cataracts in his surgical career to know very early on that he was experiencing them himself.
“I was probably 1.0-2.0+ NS and a few cortisol vacuoles. I didn’t have trouble with night driving or any of the other usual symptoms, but as a surgeon, I’m very aware of my vision — I depend on it more than most people — and I could tell there was an ever-so-slight shift.”
Throughout his decades of experience, Dr. Davies has paid close attention to the development of lenses. Although some new technologies were impressive, the tradeoffs always gave him pause, and he’d find himself looking for the next thing. While he waited for a lens — for his patients and himself — that didn’t come with so many drawbacks, Dr. Davies started using the phrase “multifocal anxiety syndrome” or MAS.
“MAS begins when you’re recommending the best lens option — usually what I would want for myself — and then explaining to patients that they may have glare and halos. I would get a grinding feeling in my stomach wondering ‘do I really want to recommend this?’ If we don’t have a good result, I feel it, but not nearly as much as my patients who will deal with it 24/7.”
“I would get a grinding feeling in my stomach wondering ‘do I really want to recommend this?’ If we don’t have a good result, I feel it, but not nearly as much as my patients who will deal with it 24/7.”
James Davies, MD
As he continued to watch and wait, Dr. Davies was intrigued by the research from RxSight® and the Light Adjustable Lens™ (LAL®). Reducing the risk of glare and halos was enough to catch his attention, but he really took notice when he began posing the question “what lens would you pick?” to surgeons and industry leaders he respected. All of them said the LAL.
Dr. Davies trusted their advice and decided to have the LAL for his own surgery. Not only that, but soon after, he decided to purchase a Light Delivery Device (LDD) for his practice as well.
Dr. Davies enlisted his friend Dr. Arturo Chayet, who was already offering the technology, to perform his cataract surgery. In early 2021, Dr. Davies had his non-dominant eye done. He was able to see patients in his own clinic the following day. Two days later, on a Friday, he returned for his second eye. Dr. Davies performed eight cataract surgeries the following Monday.
Even though he’d known to expect it, Dr. Davies was still amazed by his clarity. He could see details on the mountains he’d overlooked before. He could read the hymn book on his phone during Sunday services. He noticed the pores on loved ones’ faces. And on went the list — a list he intentionally shared with his wife Becky during their drives for his follow-up treatments. Months later, Becky chose the LAL for her own cataract surgery.
Now, Dr. Davies implants the LAL almost exclusively because “it truly is the best option for most of my patients” — an option made even better by his firsthand experience.
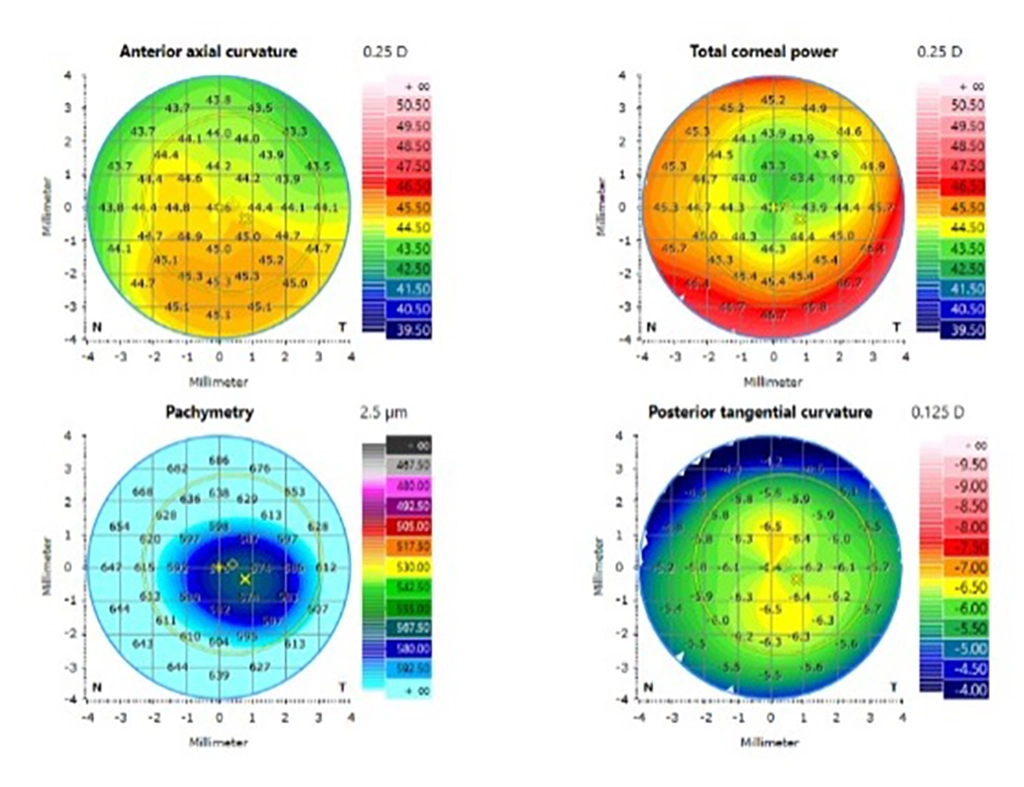
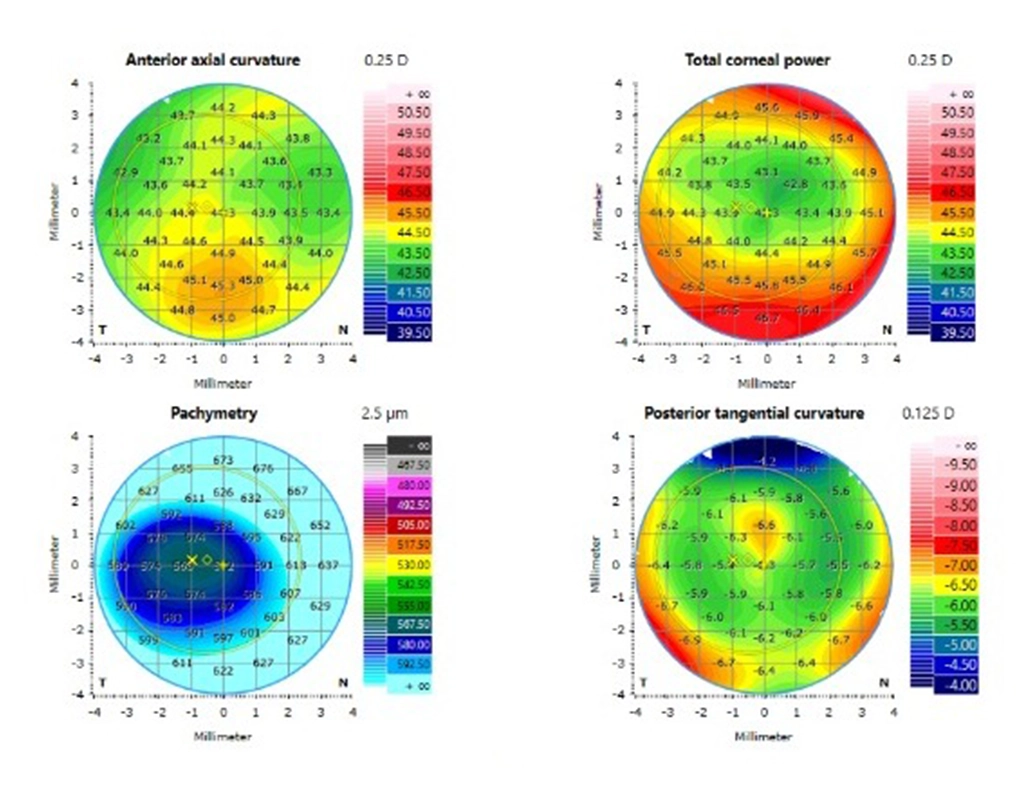
Case Study
Patient Profile
68-year -old male
OS dominant
| Post-op before LDD treatments | MR | +0.50D | +0.50 – 0.50 x 66 |
|---|
OD Post-op after LDD Lock-in
20/25
and J1+
OS Post-op after LDD Lock-in
20/15
and J3
OU Post-op after LDD Lock-in
20/16