For my father, only adjustability will do.

Dr. Bryan Monson and his father, Dr. Roland Monson, have always enjoyed a good adventure together. In early 2022, they embarked on their greatest one yet. A retired optometrist, Roland was well aware that he was experiencing cataracts, and at 77 years old, he knew it was time for surgery.
He sought out his son and ophthalmologist Dr. Bryan Monson at Monson Vision in Logan, UT for a consultation. Roland presented with months of increased difficulty with nighttime driving, three years of measurable myopic shift, decreased accommodative near point, and diminished contrast sensitivity consistent with advancing cataracts. He was also being treated for underlying keratoconjunctivitis sicca.
Roland required excellent clarity and contrast sensitivity. His active lifestyle and 66 years of dependency on glasses underscored his desire for excellent uncorrected distance vision. As an avid reader and a naturally high myope, maintaining excellent, uncorrected near vision was likewise important.
Given those circumstances, Dr. Bryan Monson recommended that his favorite optometrist, patient, and father select the Light Adjustable Lens (LAL) for his surgery.
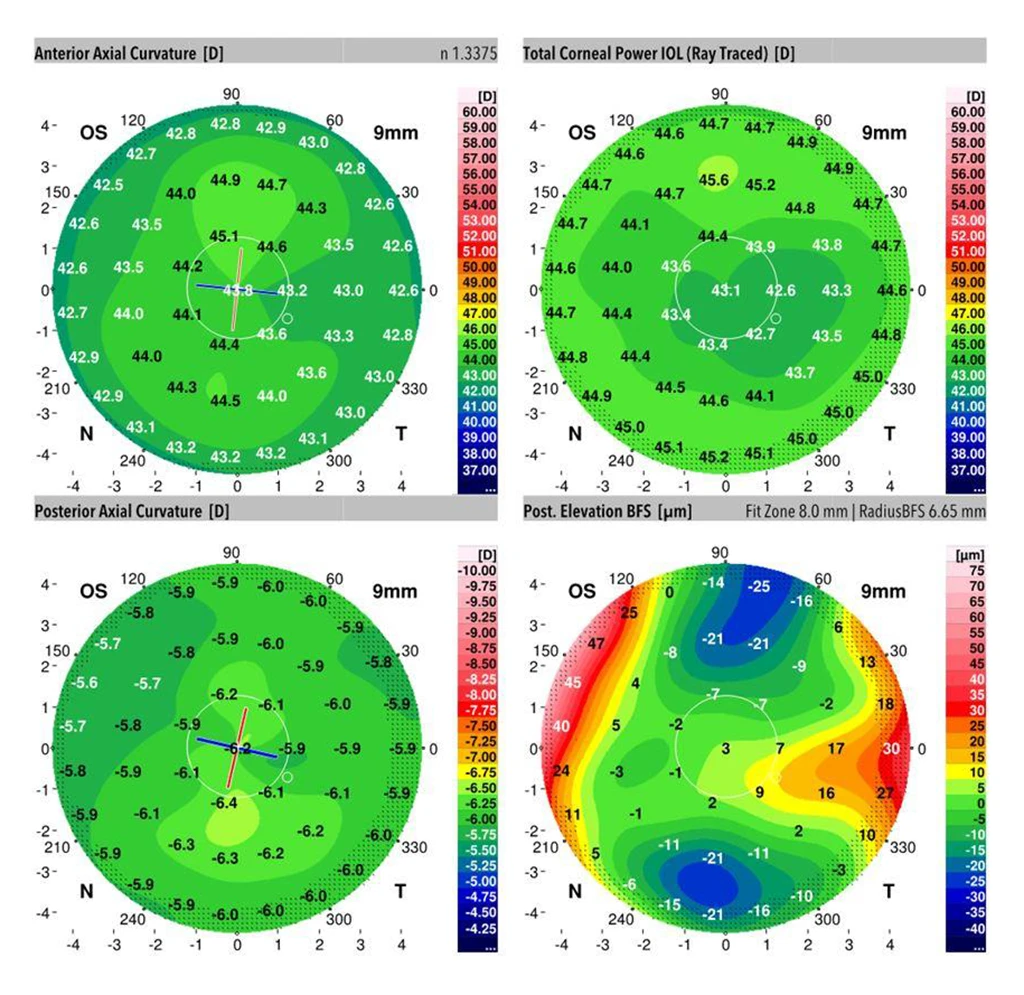
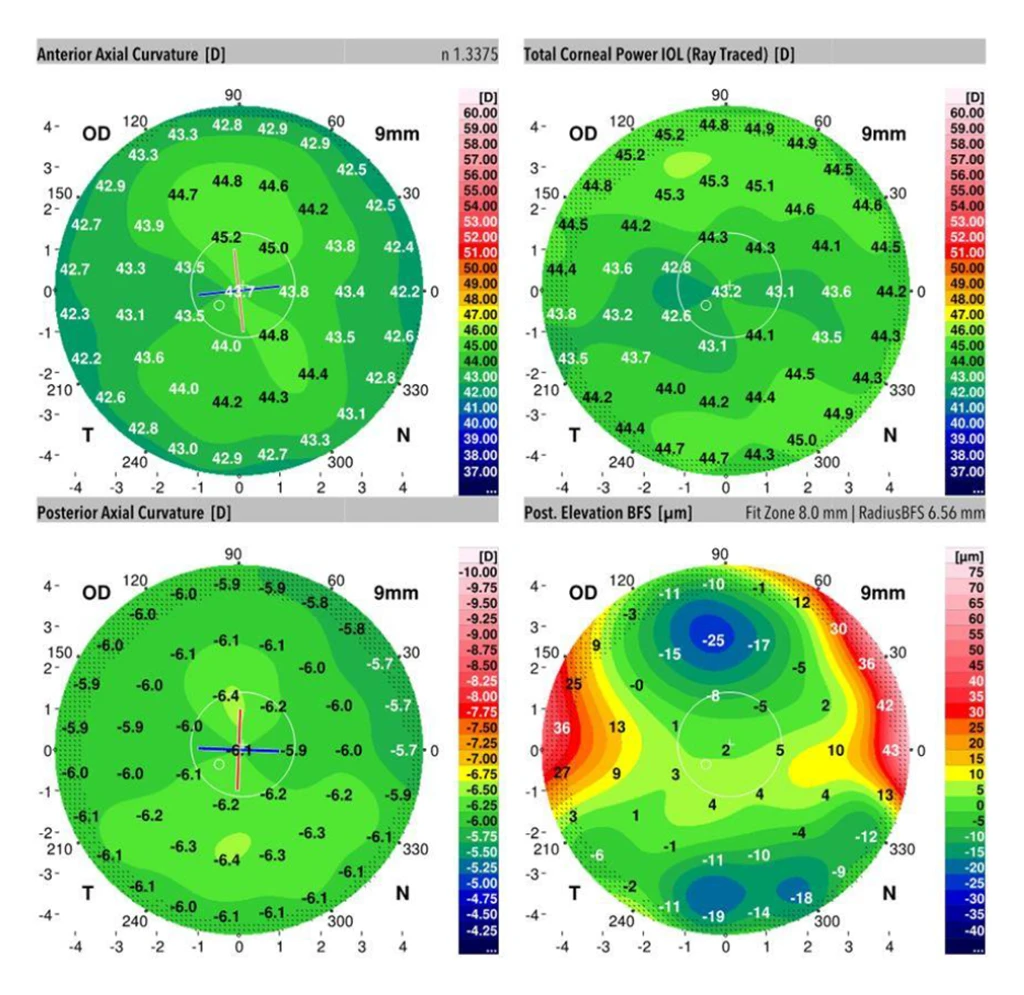
Dr. Roland Monson had nremarkable low-grade trefoil and coma higher-order aberration (HOA) at both cornea and crystalline lens locations and long axial lengths consistent with high myopia.
“The LAL technology is an important option for a wide range of cataract patients,” says Bryan Monson. “It extends the option for spectacle independence to new patient subcategories that previously have not been suitable candidates.”
Roland Monson would be one such subcategory. As a naturally high myope, he first considered two other lenses, neither of which was ideal, before he and his son settled on the LAL. Roland understood that some of the macromers in the LAL would go toward fixing his astigmatism and that he would have blended vision once the treatments were complete.
“My right eye is my distance correction. From the beginning it was phenomenally clear. I knew what to expect, but to experience the details firsthand is even more amazing. My left eye needed close range vision and to correct that astigmatism. It got steadily better, and it’s really good now,” says Dr. Monson, Sr.
Six months post lock-in and counting, both father and son are pleased with the results — and the opportunity they had to do this together.
“The LAL is an indispensable option in our full portfolio of vision restoration procedures. I have placed LAL for thousands of guest patients, neighbors, colleagues, and family members” said Dr Monson. “In our practice, patient satisfaction and spectacle independence levels are high with LAL, making it an attractive option for a wide range of patients with lens dysfunction syndrome.”

“The LAL technology is an important option for a wide range of cataract patients. It extends the option for spectacle independence to new patient subcategories that previously have not been suitable candidates.”
Bryan Monson, MD
Case Study
Patient Profile
77-year-old male
OD dominant
Surgical Plan
Same-day sequential small-incision femtosecond laser assisted cataract surgery (FLACS) was performed with 5.2mm capsulorhexis, 2.2mm tri-planar diamond keratome, 0.9mm diamond paracenteses, vertical chop technique.
| OD | OS | ||
|---|---|---|---|
| Pre-op | UCDVA | 20/70 | 20/80 |
| UCNVA | J1+ OU | ||
| MR | -4.75 + 0.75 x 118 + 2.75 = 20/40 | -5.00 + 0.50 x 066 + 2.75 = 20/40 -2 | |
| Post-op before LDD treatments | MR | -0.25 + 1.00 x 105 = 20/15 | +0.50 SPH = 20/20 |
OD Post-op after LDD Lock-in
plano sphere
20/15
OS Post-op after LDD Lock-in
-1.50 sphere
J1+
20/40